
Table of Contents
What Is Value-Based Care Billing?
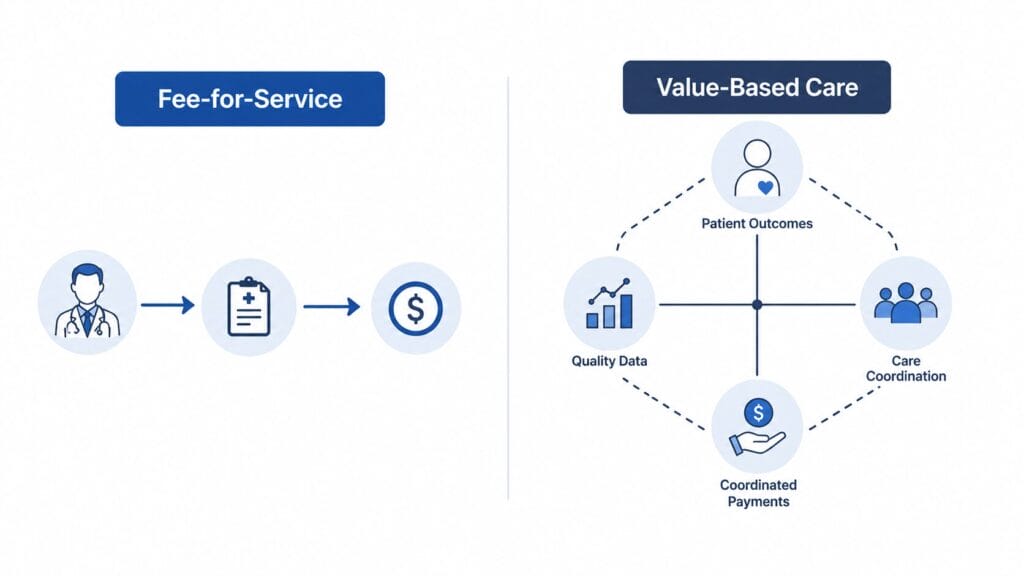
Value-based care (VBC) billing is a reimbursement model where providers are paid based on the quality and outcomes of the care they deliver, rather than the sheer number of services they perform. Under the traditional fee-for-service model, a practice gets paid for every procedure, visit, and test. Under value-based care, what matters is whether the patient got better, whether preventive benchmarks were met, and whether care was coordinated effectively.
In plain language: fee-for-service pays you for doing things. Value-based care pays you for doing things that work.
This shift affects primary care practices, specialty groups, behavioral health providers, and multi-specialty clinics alike. No corner of private medicine is untouched. Over 60% of U.S. healthcare payments now flow through value-based arrangements, and the number continues to climb as Medicare, Medicaid, and commercial insurers accelerate the transition.
of U.S. healthcare payments now through value-based arrangements
Medicare payment swing for MIPS-eligible clinicians based on 2025 scores
estimated annual revenue disadvantage for practices outside APM participation
Why Private Practices Are Most at Risk in 2026
Large hospital systems and integrated health networks built their infrastructure for value-based care years ago. They have dedicated quality reporting teams, real-time analytics platforms, and the capital to absorb the learning curve. Private practices have none of that by default.
Rural, small, and independent practices have seen the lowest participation rates in value-based payment models, and their patients have been left behind as a result. This is not a technology problem alone. It is a billing knowledge problem, a documentation problem, and in many cases a staffing problem that a capable billing partner can help resolve.
The revenue risk is not theoretical. Practices that remain on purely volume-based billing face an estimated $204,000 to $306,000 annual revenue disadvantage compared to peers participating in alternative payment models (APMs) in 2026. That figure does not account for the MIPS payment adjustment, which adds another layer of risk on top.
How the CMS 2026 Physician Fee Schedule Changes Everything
The 2026 CMS Physician Fee Schedule did not just adjust conversion factors. It created two distinct financial realities: one for practices participating in approved alternative payment models, and another for practices that are not. The gap between those two realities is measurable and grows every year.
The MIPS Payment Adjustment
The Merit-Based Incentive Payment System (MIPS) is the quality payment program that applies to most Medicare-billing providers. Based on a clinician’s 2025 performance data, CMS applies a payment adjustment in 2026 that can swing up to 9% in either direction. Positive scores earn bonuses. Poor scores or non-participation result in payment reductions applied across all Medicare claims for the year.
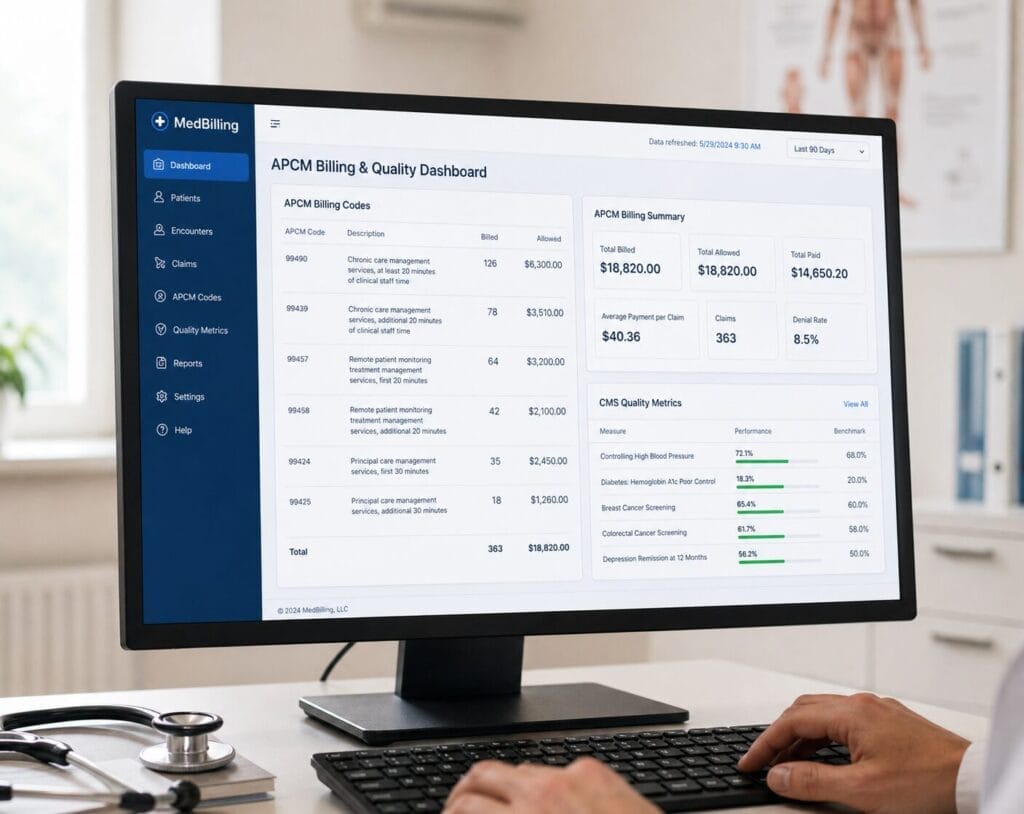
The New APCM Codes
The 2026 fee schedule introduced a set of new codes for Advanced Primary Care Management (APCM) that represent a genuine billing opportunity for qualifying practices. Unlike older chronic care management codes that required time-based thresholds, APCM codes are built around a patient’s chronic condition complexity and the level of primary care services provided.
APCM Codes at a Glance
The ACO REACH Model
For larger or growing private practices, the ACO REACH model offers another pathway into value-based care participation. REACH (Realizing Equity, Access, and Community Health) allows groups of providers to take on shared savings and shared risk through coordinated care arrangements. While this model is more complex to enter, it offers the highest potential upside for practices ready to commit to full care coordination infrastructure.
Fee-for-Service vs Value-Based Care Billing: Key Differences
Understanding the structural difference between these two models is essential before your practice can adapt its billing workflow. The contrast goes deeper than just how payments are calculated.
| Factor | Fee-for-Service | Value-Based Care |
|---|---|---|
| Payment Basis | Volume of services performed | Quality of outcomes delivered |
| Documentation Focus | Procedure and encounter-based | Outcome and quality metric-based |
| Revenue Risk | Low per claim | Performance-dependent |
| Reporting Requirements | Standard claim submission | Quality data, HEDIS, CAHPS measures |
| Upside Potential | Fixed to volume | Bonuses for high performance |
| Payer Relationships | Transactional per claim | Longitudinal and contract-based |
The critical point here is not that one model is better than the other in isolation. The issue is that most private practices are operating in both worlds simultaneously. Some payers have moved to VBC contracts while others still use fee-for-service arrangements. Running two parallel billing workflows without expertise in both is exactly where revenue leaks happen.
What Value-Based Care Billing Actually Changes in Your Practice
This is where many guides stop at theory. Here is what VBC billing changes in practical, daily terms for a private practice.
Documentation must now reflect outcomes, not just services. A visit note written purely to justify a CPT code is not sufficient under value-based care contracts. Notes must capture care coordination, patient-reported outcomes, chronic condition management, and follow-through on preventive benchmarks. This is a documentation training issue as much as it is a billing issue.
Quality data reporting is non-negotiable. Under MIPS and most commercial VBC contracts, quality measures must be submitted within specific reporting windows. Missing a reporting deadline cannot be corrected after the fact. Even a single documentation gap can reduce reimbursement or erase a quality bonus that the practice earned through excellent clinical care throughout the year.
Coding must align with what payers are actually measuring. Submitting the correct CPT code is necessary but no longer sufficient. The codes must connect to the quality metrics the payer is tracking. If a practice is managing a patient’s diabetes effectively but the documentation does not reflect the specific HEDIS measure being monitored, the payer does not see the quality performance. The practice earns nothing for care it actually delivered.
Billing timelines shift under VBC. Quality data reporting windows, annual risk adjustment reviews, and care management billing cycles operate on different timelines than traditional claims. A billing team unfamiliar with these windows will miss them regularly.
The 4 Biggest Billing Challenges Private Practices Face with VBC
Documentation Complexity
Clinical notes must now capture quality indicators alongside standard encounter information. Most billing teams were never trained on outcome-based documentation requirements, and many physicians are writing notes that fall short without knowing it.
Dual Workflow Management
A practice running some payers on fee-for-service and others on VBC contracts must manage two fundamentally different billing workflows in parallel. Without clear systems, claims fall through the cracks at the intersection.
Quality Reporting Deadlines
MIPS reporting windows, HEDIS measure submission periods, and annual risk adjustment reviews all operate on fixed calendars. Missing a single window can mean thousands of dollars in lost bonuses or earned payment adjustments that cannot be recovered.
Staff Training Gaps
Billing staff trained on traditional RCM have a different skill set than what VBC requires. The gap in knowledge around outcome-based coding, quality measure alignment, and APM contract requirements is real and costly when left unaddressed.
How to Prepare Your Practice for Value-Based Care Billing
Transitioning to value-based care billing does not require overhauling your practice overnight. It requires a structured, sequenced approach that identifies your current gaps and closes them without disrupting cash flow. Here is a practical roadmap.
Audit your current billing workflow against VBC requirements
Start with a detailed review of how your current claims are documented, submitted, and followed up. Identify which payers have moved to VBC contracts and which are still fee-for-service. This audit becomes the baseline for every improvement that follows.
Identify which payers have moved to VBC contracts
Not every payer operates on the same model. Map your payer mix against your contracts and determine exactly which ones are measuring quality metrics, which are applying payment adjustments, and which ones have upcoming VBC contract renewals.
Ensure documentation captures quality metrics at every visit
Work with your clinical staff to update note templates and workflows so that every patient encounter documents the data points your VBC payers are measuring. This is a documentation process change, not a technology purchase.
Evaluate your MIPS participation and current performance score
If you are Medicare-eligible and not actively managing your MIPS score, you are almost certainly leaving money on the table or absorbing a payment penalty without knowing it. Pull your current score and measure it against the 2025 performance thresholds.
Assess APCM code eligibility across your patient panel
Review your chronic care patient population against the eligibility criteria for G0556, G0557, and G0558. Many practices have qualifying patients they are not billing APCM codes for, leaving substantial monthly revenue uncaptured.
Partner with a billing company that understands VBC from the inside
The most effective shortcut is working with an RCM partner that already has VBC expertise built into its process. This eliminates the learning curve, protects cash flow during the transition, and ensures reporting deadlines are never missed.
How HS MED Solutions Supports Value-Based Care Billing
HS MED Solutions is not a software platform or an automated clearinghouse. We are a hands-on revenue cycle management partner with 25 years of billing experience across 40 specialties, including primary care, multi-specialty groups, and behavioral health practices navigating VBC transitions right now.
- Documentation review aligned to quality metrics and VBC contracts
- APCM code eligibility assessment across your patient panel
- 24-hour claim turnaround with full transparency reporting
- Specialty-specific expertise across 40+ practice types
- MIPS score tracking and quality reporting support
- Dual workflow management for mixed FFS and VBC payer environments
- Denial management and underpayment recovery
- Dedicated account team, not a rotating support desk
Frequently Asked Questions
The following questions cover what private practice owners and administrators ask most often when navigating the shift to value-based care billing.
Value-based care billing is a reimbursement model where providers are paid based on the quality and outcomes of care delivered, not the number of services performed. It includes programs like MIPS, ACO arrangements, and payer-specific quality contracts that tie payment adjustments to documented clinical performance.
Practices that do not adapt to VBC models face two types of revenue impact. First, they risk negative payment adjustments of up to 9% on Medicare revenue through MIPS non-participation. Second, they miss new billable revenue opportunities from codes like APCM (G0556, G0557, G0558) that qualifying practices can bill monthly for chronic care patients. The combined annual difference can exceed $200,000 for a mid-size private practice.
MIPS stands for Merit-Based Incentive Payment System. It is the CMS quality payment program that applies to the majority of clinicians who bill Medicare. Practices that meet the low-volume threshold are subject to MIPS, and non-participation results in a negative payment adjustment applied across all Medicare claims for the following payment year. Participation is not technically mandatory, but the cost of non-participation is a guaranteed penalty.
APCM codes (G0556, G0557, G0558) are CMS codes introduced in 2026 for Advanced Primary Care Management services. They allow qualifying primary care practices to bill for ongoing chronic care coordination, 24/7 access support, and care planning without requiring the time-based thresholds that older chronic care management codes used. Eligibility depends on the patient's chronic condition complexity and the practice's designation as a primary care provider. A billing partner with VBC expertise can complete an eligibility audit across your patient panel.
Yes, with the right sequence. The key is not attempting a wholesale switch at once. A structured transition starts with a billing audit, moves to documentation workflow updates, then to quality reporting implementation, and finally to APCM or APM code integration. Working with an experienced RCM partner allows this to happen in stages so revenue stays stable throughout the process. Practices that try to manage this internally without dedicated VBC expertise typically experience cash flow gaps during the transition.
Value-based care billing is not arriving. It is already here, and it is already affecting how much your practice collects. Every month without a strategy is a month of potential revenue being left behind or penalties being absorbed without awareness. HS MED Solutions works with private practices across every specialty to close that gap, from MIPS reporting to APCM billing to complete RCM support built for the value-based environment.



4 Responses
You ought to take part in a contest for one of the best sites
on the net. I am going to highly recommend this site!
I am actually glad to read this web site posts which contains lots
of helpful facts, thanks for providing these kinds of statistics.
I was recommended this blog by my cousin. I am not sure whether this post is written by him as nobody else know
such detailed about my trouble. You’re wonderful!
Thanks!
No matter if some one searches for his required thing, therefore
he/she needs to be available that in detail, so that thing is maintained over here.