Cardiology CPT codes are the foundation of every reimbursement claim your practice submits. Selecting the wrong code on a cardiac catheterization or echocardiography claim costs your practice real money. As a result, cardiology billing teams, practice managers, and cardiologists all need a reliable, up-to-date reference that goes beyond a simple list. This guide covers every major category of cardiology billing codes, explains how to use them correctly, and highlights every critical 2026 update that affects your claims starting January 1, 2026.
Furthermore, 2026 brought the most significant cardiology coding changes in more than a decade. Specifically, the AMA issued 288 new codes, deleted 84 codes, and revised 46 code descriptions across the CPT manual. PCI codes changed completely. A new AI-assisted imaging code gained Category I status. Remote monitoring rules expanded. Therefore, practices that have not updated their charge master and coder training for 2026 are already submitting incorrect claims.
Additionally, this guide covers cardiology CPT codes across all major procedure categories: ECG, echocardiography, stress testing, cardiac catheterization, percutaneous coronary intervention, electrophysiology, pacemakers and devices, nuclear cardiology, coronary CT angiography, and remote physiologic monitoring. Each section also includes the most common billing errors and the documentation your team needs to support every claim. HS MED Solutions has provided specialized cardiology medical billing services for more than 25 years, and consequently, every recommendation in this guide reflects real-world billing experience across all cardiology subspecialties.
Understanding the Cardiology CPT Code Framework
Before using specific cardiology CPT codes, your billing team needs to understand how the AMA organizes cardiovascular procedure codes. The primary cardiovascular range runs from 92920 to 93799. However, cardiology billing codes also appear in radiology (75571 to 75577 for coronary CT), nuclear medicine (78451 to 78499), and surgery sections for device implantation. Therefore, a cardiologist’s charge ticket may pull from four separate CPT sections on a single day.
Specifically, the AMA groups cardiovascular CPT codes into these primary categories:
- Electrocardiography (ECG/EKG): 93000 to 93042
- Cardiovascular stress testing: 93015 to 93018
- Echocardiography: 93303 to 93356
- Cardiac catheterization: 93451 to 93572
- Electrophysiology studies and ablation: 93600 to 93662
- Pacemaker and implantable device services: 33206 to 33270
- Percutaneous coronary intervention (PCI): 92920 to 92945 restructured for 2026
- Nuclear cardiology: 78451 to 78499
- Coronary CT angiography: 75571 to 75577, new code 75577 added for 2026
- Remote physiologic monitoring (RPM): 99453, 99454, 99457, 99458, 99470 revised for 2026
Why Modifier Knowledge Is Inseparable from CPT Code Knowledge
Cardiology CPT codes almost always require modifiers to specify how a service was delivered. Modifier 26 indicates the professional component only, meaning the cardiologist provided interpretation but not technical performance. The modifier TC covers the technical component only. Modifier 59 identifies distinct procedural services performed on the same day. The vessel modifiers LD, LC, RC, LM, and RI are required on every PCI claim to identify the treated coronary artery. Therefore, selecting the correct cardiology billing code without the correct modifier produces a claim that pays at the wrong rate or is denied completely.
Furthermore, NCCI edits define which cardiology procedure codes can be billed together and which are considered bundled. CMS updates these edits quarterly. Consequently, billing teams must review NCCI edit updates every quarter and adjust claim submission logic when bundling rules change for high-volume cardiology codes.
HS MED Solutions Tip: We run every cardiology claim through an automated NCCI edit scrubber before submission. This single step prevents the majority of bundling denials that cardiology practices experience from in-house billing teams.
Electrocardiography CPT Codes 93000 to 93042
ECG codes are the most frequently billed cardiology billing codes in outpatient practice. They are also the most frequently miscoded because three distinct scenarios exist: the complete service, the technical component only, and the professional component only. Specifically, the scenario depends on who performs the ECG and who interprets it.
| CPT Code | Description | Correct Billing Scenario |
| 93000 | ECG with at least 12 leads complete service (tracing + interpretation + report) | One provider performs AND interprets the ECG in the same setting |
| 93005 | ECG tracing and recording only a technical component | Technician performs the tracing; a separate provider interprets |
| 93010 | ECG interpretation and report only professional component | A cardiologist interprets an ECG performed at a different facility; do not add modifier 26 |
| 93040 | Rhythm ECG with interpretation and report | Shorter rhythm strip for arrhythmia monitoring includes interpretation |
| 93041 | Rhythm ECG tracing only | Technical component for rhythm strip interpreter bills 93042 separately |
| 93042 | Rhythm ECG interpretation and report only | Professional component for rhythm strip pair with 93041 from the technical site |
The Most Common ECG Billing Error
Audit Alert: Never bill 93000 and 93010 on the same claim for the same patient on the same date. Code 93000 already includes the interpretation component. Billing both creates a duplicate billing error and triggers an automatic NCCI denial. Additionally, modifier 26 should never be appended to code 93010, because 93010 is already the professional-component-only code.
Furthermore, if your practice bills ECGs performed in your office but sent to a remote cardiologist for interpretation, split the billing correctly. Bill 93005 (technical component) from the office and 93010 (professional component) from the interpreting cardiologist. This split-billing scenario is common in multi-site and telehealth cardiology arrangements and represents one of the most audited ECG billing patterns.
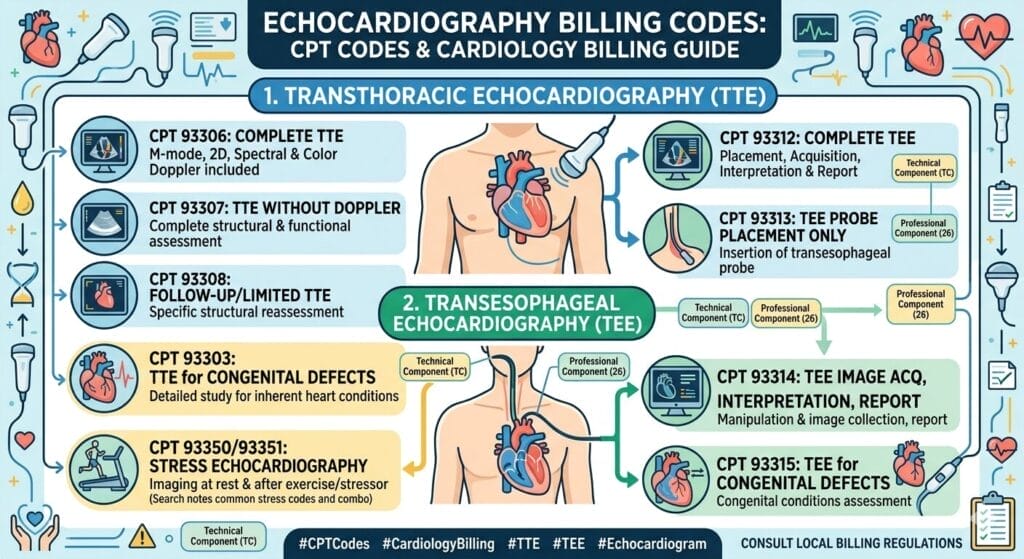
Echocardiography CPT Codes 93303 to 93356
Echocardiography cardiology billing codes carry some of the highest audit rates among all cardiovascular procedure codes. Specifically, payers scrutinize echo claims because the difference between a complete study (93306) and a limited study (93308) represents a meaningful reimbursement gap. Therefore, documentation must clearly support whichever echocardiography code your practice submits.
Transthoracic Echocardiography (TTE) Codes
| CPT Code | Description | Documentation Required |
| 93306 | Complete TTE with spectral and color Doppler | All cardiac structures, chamber measurements, and Doppler flows in every standard view must be documented |
| 93307 | Complete TTE without Doppler | Same structural documentation as 93306, no Doppler component billed |
| 93308 | Follow-up or limited TTE | Specific clinical indication required, do not routinely downcode from 93306 |
| 93312 | Transesophageal echo (TEE) complete | Full image acquisition, probe insertion, interpretation report, all views required |
| 93314 | TEE image acquisition only (technical component) | Use when the cardiologist interprets separately bill 93316 for the professional component |
| 93316 | TEE interpretation and report only (professional component) | Pair with 93314 from the technical site |
| 93350 | Stress echo rest and exercise or pharmacologic stress | Document stress protocol, rest, and stress images are both required |
| 93351 | Stress echo with contrast | Same as 93350, also document the contrast agent used and the clinical indication |
| 93303 | Congenital TTE complete (pediatric) | Use for congenital anomaly evaluation, do not substitute 93306 for congenital cases |
| 93304 | Congenital TTE follow-up or limited | Document congenital indication not interchangeable with 93308 |
The Overcoding Risk That Triggers CMS Audits
Audit Alert: Billing 93306 (complete TTE) requires documentation of all standard cardiac views with measurements. If any component is missing, the correct cardiology billing code is 93308 (limited). Overcoding from limited to complete is among the top audit triggers in outpatient echocardiography. CMS contractors specifically target this pattern in post-payment reviews.
Additionally, contrast agents used during echocardiography, for example, Definity or Lumason, do not change the CPT code for standard TTE. Code 93306 remains correct for a complete TTE with contrast. However, for stress echocardiography, code 93351 specifically captures contrast use and reimburses at a higher rate than 93350. Therefore, always document contrast agent name, volume, and clinical indication when billing 93351.
Cardiovascular Stress Test CPT Codes 93015 to 93018
Stress testing cardiology CPT codes require careful attention because the service can be billed as a complete package or split between technical and professional components. Specifically, who performs the test, who supervises it, and who interprets the results determines which stress test code your practice should use.
| CPT Code | Description | Billing Scenario |
| 93015 | Complete cardiovascular stress test supervision, tracing, and report | One cardiologist performs, supervises, and interprets same setting |
| 93016 | Cardiovascular stress test: physician supervision only | Cardiologist supervises but another provider interprets |
| 93017 | Cardiovascular stress test tracing only (technical component) | The technician performs the test cardiologist interprets separately |
| 93018 | Cardiovascular stress test interpretation and report only | Professional component cardiologist interprets a test performed elsewhere |
Critical Bundling Rules for Stress Test Codes
Audit Alert: Do not bill 93015 alongside 93351 (stress echo) on the same date for the same patient. Code 93351 already includes the stress test component. Billing both creates a bundling error subject to automatic NCCI denial. Similarly, do not bill 93015 with nuclear stress test code 78452. Code 78452 includes the stress component, so billing 93015 additionally is a duplicate billing error.
Furthermore, payers frequently require prior authorization for nuclear stress tests and pharmacologic stress testing. Therefore, confirm PA requirements for each payer before scheduling these procedures. Additionally, documentation for every stress test must include the clinical indication, the protocol used (treadmill versus pharmacologic), patient response during the test, and a complete written interpretation with findings.
Cardiac Catheterization CPT Codes 93451 to 93572
Cardiac catheterization cardiology billing codes are high-value, high-complexity, and consistently among the highest audit-risk codes in the cardiovascular section. Moreover, the distinction between right heart, left heart, and combined catheterization, and whether coronary angiography is included, determines the correct primary code. Selecting the wrong level of service on a cardiac catheterization claim represents both a compliance risk and a revenue loss.
| CPT Code | Description | Key Notes |
| 93451 | Right heart catheterization all required elements | Includes right atrium, right ventricle, pulmonary artery, and wedge pressure |
| 93452 | Left heart catheterization with coronary angiography | Most common single-vessel diagnostic cath code |
| 93453 | Combined right and left heart catheterization | Both sides in one session do not bill 93451 and 93452 separately |
| 93454 | Coronary angiography without left heart catheterization | For selective coronary imaging when LHC is not performed |
| 93456 | Right heart cath with coronary angiography | Right side plus coronary angiography in one session |
| 93457 | Right heart cath with coronary angiography and bypass grafts | Adds bypass graft imaging to 93456 |
| 93458 | Left heart cath with coronary angiography and left ventriculography | Comprehensive left-side cath including LV gram |
| 93459 | Left heart cath with coronary angiography, LV gram, and bypass grafts | Most comprehensive left-side code includes graft imaging |
| 93460 | Combined right and left heart cath with coronary angiography | Full combined procedure code |
| 93461 | Combined right and left heart cath with coronary angiography and bypass grafts | The highest-level cath code includes bypass graft imaging |
Add-On Codes for Cardiac Catheterization
Additionally, several add-on cardiology billing codes are frequently billed alongside the primary catheterization code. These add-ons capture additional diagnostic work performed during the same session:
- 93567 – Supravalvular aortic angiography (add-on to primary cath code)
- 93568 – Pulmonary angiography during catheterization (add-on code)
- 93571 – Fractional flow reserve (FFR), initial vessel (billing rules updated for 2026)
- 93572 – FFR, each additional vessel (add-on code)
- 92978 – Intravascular ultrasound (IVUS), initial vessel (verify bundling rules before billing)
- 92979 – IVUS, each additional vessel (add-on)
Audit Alert: IVUS codes 92978 and 92979 carry bundling edits with several PCI codes. Verify NCCI edits quarterly before billing IVUS alongside PCI. Furthermore, some payers require a separate prior authorization for IVUS, independent of the PA obtained for the catheterization itself.
Percutaneous Coronary Intervention (PCI) CPT Codes 2026 Complete Overhaul
PCI cardiology CPT codes experienced the most significant restructuring in the entire 2026 update cycle. Specifically, the AMA deleted six long-standing add-on codes that practitioners used to report additional branch vessel work during PCI. That work now integrates into revised primary PCI codes. Furthermore, the AMA introduced two new Category I codes, 92930 and 92945, to better capture complex PCI and chronic total occlusion revascularization. Consequently, practices that have not updated their PCI coding workflows are submitting incorrect claims on every PCI encounter in 2026.
The Deleted Add-On Codes Every Biller Must Know
Audit Alert: Codes 92921, 92925, 92929, 92934, 92938, and 92944 were permanently deleted on January 1, 2026. Any claim using these codes in 2026 will be denied on submission. Update your charge master, EHR code sets, and coder reference sheets immediately. There is no grace period for deleted codes.
| CPT Code | Description (2026) | 2026 Change Status |
| 92920 | PTCA single or multiple major coronary artery or branch(es) | REVISED branch work is now bundled into the primary code |
| 92924 | Coronary atherectomy with or without angioplasty, single or multiple branches | REVISED branch add-on deleted and bundled in |
| 92928 | Stent placement with angioplasty single major coronary artery or branch(es) | REVISED branch add-on deleted |
| 92930 | Complex PCI bifurcation lesion or multiple lesions requiring main artery and side branch intervention | NEW CODE 2026. ~20% more RVU credits than 92928. |
| 92933 | Atherectomy plus stent with angioplasty, single or multiple branches | REVISED branch work bundled in |
| 92937 | PCI on bypass graft (not LIMA to LAD) | REVISED wording |
| 92941 | PCI during acute MI | REVISED wording |
| 92943 | Chronic total occlusion PCI | RETAINED is now distinct from the new code 92945 |
| 92945 | CTO revascularization of new complex chronic total occlusion code | NEW CODE 2026. Captures resource intensity of complex CTO procedures. |
| 92921, 92925, 92929, 92934, 92938, 92944 | Branch vessel add-on codes (previously used for extra branch work) | DELETED January 1, 2026. Do not use. |
Vessel Modifiers Required on Every PCI Claim
Medicare and most commercial payers require vessel-specific modifiers on all PCI cardiology billing codes. Specifically, these modifiers identify which coronary artery received treatment:
| Modifier | Coronary Vessel |
| LD | Left anterior descending coronary artery (LAD) |
| LC | Left circumflex coronary artery (LCx) |
| RC | Right coronary artery (RCA) |
| LM | Left main coronary artery |
| RI | Ramus intermedius coronary artery |
Furthermore, for new complex PCI code 92930, documentation must clearly describe the bifurcation anatomy treated, all lesion locations, specific vessels and segments involved, and the interventional strategy used for both the main vessel and the side branch. Vague documentation does not support 92930 and creates a downcode risk on audit.
2026 Update: Code 92930 provides approximately 20% more RVU credits than standard stent code 92928. However, clinical documentation must specifically describe bifurcation involvement or multiple distinct lesion treatment. A cardiology practice that performs 50 complex PCI procedures per month and correctly identifies and codes 92930 where appropriate can recover significant additional revenue that was previously left on the table.
Electrophysiology Study and Ablation CPT Codes 93600 to 93662
Electrophysiology cardiology billing codes are the most complex category in the entire cardiovascular section. EP procedures combine primary procedure codes with multiple add-on codes for mapping, intracardiac imaging, and additional ablation targets. Therefore, billing an EP encounter correctly requires coders with specific electrophysiology training, not just general cardiology coding knowledge.
EP Study Codes
| CPT Code | Description | Key Notes |
| 93619 | Comprehensive EP study without attempted arrhythmia induction | Standard comprehensive EP includes atrial and ventricular recording and pacing |
| 93620 | Comprehensive EP study with attempted arrhythmia induction and treatment | The highest-level diagnostic EP includes an arrhythmia induction attempt |
| 93621 | EP study with left atrial pacing and recording (add-on) | Add-on to 93620 document transseptal access |
| 93622 | EP study with left ventricular pacing and recording (add-on) | Add-on to 93620 document retrograde aortic or transseptal access |
| 93600 | Bundle of His recording only | Rarely billed standalone, typically part of a comprehensive EP study |
| 93602 | Intra-atrial recording only | Standalone intra-atrial recording without comprehensive EP study |
| 93610 | Intra-atrial pacing only | Standalone atrial pacing is often used in EP diagnostic workup |
| 93612 | Intraventricular pacing only | Standalone ventricular pacing document clinical indication |
Cardiac Ablation CPT Codes
| CPT Code | Description | Critical Billing Note |
| 93651 | Ablation of atrial flutter or atrial tachycardia (not AFib) | Includes comprehensive EP evaluation, do not also bill 93620 |
| 93652 | Ablation of AV node (with pacemaker implant) | Includes pacemaker insertion do not separately bill pacemaker code |
| 93653 | Ablation of supraventricular tachycardia (SVT, not AFib or atrial flutter) | Includes comprehensive EP evaluation |
| 93654 | Ablation ventricular tachycardia (VT) | High-risk procedure requires detailed pre- and post-procedure documentation |
| 93655 | Additional arrhythmia substrate ablation (add-on) | Add-on bill for each additional arrhythmia site alongside the primary ablation code |
| 93656 | AFib ablation including pulmonary vein isolation (PVI) | Includesa comprehensive EP evaluation, the most common AFib ablation code |
| 93657 | Additional linear or focal ablation for AFib (add-on) | Add-on to 93656 for ablation lines beyond PVI |
| 93662 | Intracardiac echocardiography (ICE) during EP or ablation (add-on) | Bill alongside primary ablation or EP code document ICE findings separately |
Audit Alert: AFib ablation code 93656 already includes a comprehensive EP evaluation. Therefore, billing 93619 or 93620 on the same date as 93656 creates a duplicate billing error subject to automatic NCCI denial. This is one of the most common EP billing errors that cardiology practices make.
Pacemaker and Implantable Device CPT Codes
Pacemaker and ICD cardiology billing codes consistently appear in OIG Work Plans as high-priority audit targets. Consequently, documentation for every device implantation must include the clinical indication, device model and serial number, lead positions, fluoroscopy time, and post-implant device testing results. Incomplete documentation is the primary reason pacemaker and ICD claims fail post-payment audit.
Device Implantation Codes
| CPT Code | Description | Chamber Configuration |
| 33206 | Pacemaker insertion, single chamber (atrial lead) | One atrial lead |
| 33207 | Pacemaker insertion, single chamber (ventricular lead) | One ventricular lead |
| 33208 | Pacemaker insertion dual chamber | Both atrial and ventricular leads |
| 33212 | Pacemaker pulse generator insertion only single chamber | Generator replacement, existing lead retained |
| 33213 | Pacemaker pulse generator insertion only dual chamber | Generator replacement: existing leads retained |
| 33214 | Upgrade from a single to a dual-chamber pacemaker | Add a lead to an existing single-chamber system |
| 33221 | Pacemaker insertion multiple leads (CRT-P) | Three or more leads for a cardiac resynchronization pacemaker |
| 33230 | ICD insertion dual chamber | ICD with two leads |
| 33231 | ICD insertion multiple leads (CRT-D) | ICD with three leads biventricular pacing configuration |
| 33240 | ICD insertion single chamber | ICD with one lead |
| 33270 | Subcutaneous ICD (S-ICD) insertion | No transvenous leads specific to the subcutaneous ICD system |
Device Follow-Up and Remote Monitoring Codes
Additionally, device management cardiology billing codes are billed separately from implantation codes. Therefore, your practice needs a dedicated workflow to capture these recurring revenue codes:
- 93279 – Single chamber pacemaker programming (in-person)
- 93280 – Dual chamber pacemaker programming (in-person)
- 93281 – CRT-P programming (in-person)
- 93285 – ICD programming (in-person)
- 93294 – Remote monitoring of pacemaker 90-day period, single chamber
- 93296 – Remote monitoring of ICD 90-day period
- 93297 – Remote monitoring of CRT-P 90-day period
2026 Update: Remote monitoring codes 93294 and 93296 require documentation of the monitoring period dates, the data received, and evidence that a cardiologist or qualified clinical staff member reviewed the transmitted data. A 90-day monitoring period with no documented data review makes every remote monitoring claim indefensible on audit.
Nuclear Cardiology CPT Codes 78451 to 78499
Nuclear cardiology billing codes involve imaging with radioactive tracers to evaluate myocardial perfusion and cardiac function. These codes carry high reimbursement values and appear as specific audit targets in multiple consecutive OIG Work Plans. Therefore, complete documentation is not optional; it is a compliance requirement for every nuclear cardiology claim your practice submits.
| CPT Code | Description | Key Documentation Requirement |
| 78451 | Myocardial perfusion SPECT single study (rest or stress) | Injection protocol, stress type, tracer used, all 17 wall segments reported |
| 78452 | Myocardial perfusion SPECT multiple studies (rest and stress) | Both rest and stress images required full segmental wall motion analysis |
| 78453 | Myocardial perfusion planar single study | Older technique verify payer coverage before billing |
| 78454 | Myocardial perfusion planar multiple studies | Rest and stress planar images planar technique documentation |
| 78459 | Myocardial PET metabolic evaluation (FDG) | PET scanner required tracer name and uptake pattern documentation required |
| 78491 | Myocardial PET perfusion, single study | Rest or stress PET-specific acquisition requirements |
| 78492 | Myocardial PET perfusion, multiple studies | Both rest and stress PET images with clinical correlation |
| 78472 | Cardiac blood pool imaging (MUGA) gated equilibrium | Ejection fraction calculation and regional wall motion assessment required |
| 78473 | MUGA multiple studies (rest and stress) | Rest and stress MUGA with EF documented at each stage |
| 78499 | Unlisted cardiovascular nuclear medicine procedure | Requires individual payer pre-approval before submitting any claim |
Audit Alert: Nuclear stress test code 78452 must never be billed with standard stress test code 93015 on the same date. Code 78452 includes the stress component. Billing both is a bundling error that produces automatic denial. This is the most common nuclear cardiology billing error across all practice types.
Coronary CT Angiography CPT Codes Including New AI Code 75577
Coronary CT angiography has grown rapidly as a first-line diagnostic tool for coronary artery disease. Furthermore, the 2026 CPT update added a new Category I code specifically for AI-assisted coronary plaque analysis, a major development for cardiology practices that use advanced imaging technology.
| CPT Code | Description | 2026 Status |
| 75571 | CT heart coronary calcium quantification only (Agatston score) | Established unchanged for 2026 |
| 75572 | CCTA cardiac structure and morphology without contrast | Established unchanged |
| 75573 | CCTA with contrast, cardiac structure and morphology | Established unchanged |
| 75574 | CCTA with contrast cardiac structure, morphology, and coronary angiography | Established most comprehensive cardiac CT code |
| 75577 | AI-assisted coronary plaque analysis performed with CCTA | NEW Category I Code 2026. Replaces prior Category III experimental code. Payers must now establish formal coverage policies. |
2026 Update: Code 75577 gaining Category I status means Medicare and commercial payers must now create formal reimbursement policies for AI-assisted plaque analysis. However, individual payer implementation timelines vary. Therefore, verify coverage and obtain any required prior authorization before billing 75577 for the first time with each payer in your contract portfolio.
Remote Physiologic Monitoring (RPM) CPT Codes 2026 Changes
Remote physiologic monitoring represents a growing revenue stream for cardiology practices managing heart failure, hypertension, and arrhythmia patients. However, RPM cardiology billing codes require strict compliance with time thresholds, patient consent documentation, and data review records. Moreover, 2026 brought meaningful revisions that expand billing opportunities for practices that implement RPM correctly.
| CPT Code | Description | 2026 Change |
| 99453 | RPM device setup and patient education (one-time per device) | Unchanged bill once per device when monitoring begins |
| 99454 | RPM device supply with daily recording or transmission (30-day period) | REVISED 2026: Now covers 2–15 days in a 30-day period. Previously required 16 days minimum. |
| 99457 | RPM treatment management first 20 minutes per month | Unchanged physician or qualified healthcare professional time |
| 99458 | RPM treatment management each additional 20 minutes per month | Unchanged add-on to 99457 |
| 99470 | RPM treatment management requiring real-time patient interaction | NEW CODE 2026. Requires documented real-time interaction with patient or caregiver during the monitoring period. |
Specifically, the revised threshold for 99454 drops from a 16-day minimum to a 2 to 15-day range, benefiting practices whose patients intermittently miss device uploads. Previously, a patient who uploaded only 12 days of data in a month meant the practice could not bill 99454 at all. Under the 2026 revision, your practice can now bill 99454 for that same patient. Consequently, practices with large remote monitoring programs should recalculate their RPM revenue projections upward for 2026.
Audit Alert: RPM claims require documented patient consent, device type, specific monitoring dates, data reviewed, and total time spent on clinical management. Billing RPM cardiology billing codes without this documentation makes every RPM claim vulnerable to post-payment audit recovery by Medicare and commercial payers.
Cardiology Modifier Quick Reference
Modifiers are required on most cardiology CPT codes to specify the scope of service, the component billed, or the clinical circumstance. Specifically, using the wrong modifier or omitting a required modifier is one of the most common causes of cardiology claim denials and post-payment audit findings. Therefore, every cardiology billing team needs an up-to-date modifier reference reviewed at least annually.
| Modifier | Meaning | Common Cardiology Use Case |
| 26 | Professional component only | A cardiologist interprets an echo or nuclear study performed at another facility. |
| TC | Technical component only | Facility bills for equipment and technical staff no physician interpretation included |
| 59 | Distinct procedural service | Two separate cardiology procedures on the same date, each clinically distinct |
| XE | Separate encounter | Services from two separate patient encounters on the same date |
| XS | Separate structure | Procedures on anatomically distinct structures, for example, two different coronary arteries |
| XP | Separate practitioner | Services by two different practitioners on the same date of service |
| XU | Unusual non-overlapping service | Service that does not overlap the usual components of the primary procedure |
| 25 | Significant, separately identifiable E&M on the same day as the procedure | Office visit on same day as ECG or minor cardiology procedure |
| 50 | Bilateral procedure | Bilateral cardiac imaging rare in cardiology but used for specific nuclear studies |
| LD | Left anterior descending coronary artery | Required on all PCI claims, vessel identification modifier |
| LC | Left circumflex coronary artery | Required on all PCI claims vessel identification modifier |
| RC | Right coronary artery | Required on all PCI claims, vessel identification modifier |
| LM | Left main coronary artery | Required on PCI claims involving the left main |
| RI | Ramus intermedius coronary artery | Required when ramus intermedius receives PCI treatment |
| 57 | Decision for major surgery | E&M service the day before or day of a procedure within a global surgical period |
The Eight Most Costly Cardiology CPT Code Billing Errors
Even experienced billing teams make predictable errors on cardiology claims. Specifically, these eight errors account for the large majority of preventable cardiology billing problems. Furthermore, understanding them before they occur is significantly less costly than correcting denials, audits, or post-payment recovery demands afterward.
Errors 1 Through 4 Bundling and Code-Level Errors
- Bundling echo with stress test: Never bill 93306 (standard echo) alongside 93350 or 93351 (stress echo) on the same date. Stress echo codes include a cardiac imaging component that creates an automatic NCCI bundling conflict.
- Using deleted PCI add-on codes in 2026: Codes 92921, 92925, 92929, 92934, 92938, and 92944 were deleted on January 1, 2026. Furthermore, there is no grace period; every claim using these codes in 2026 will be denied on submission.
- Missing vessel modifiers on PCI claims: Medicare requires LD, LC, RC, LM, or RI on all PCI cardiology billing codes. Claims without vessel modifiers receive automatic rejection or denial from Medicare.
- Billing comprehensive EP study with ablation: Ablation codes 93651 through 93656 include comprehensive EP evaluation. Therefore, also billing 93619 or 93620 on the same date creates a duplicate billing error that triggers an NCCI denial.
Errors 5 Through 8: Documentation and Compliance Errors
- Underdocumenting nuclear stress tests: SPECT imaging code 78452 requires documentation of injection protocol, stress type and duration, all 17 myocardial segments, tracer type, and a complete written interpretation. Missing any element creates a serious audit vulnerability.
- Billing 93000 and 93010 together: These codes represent the same ECG service split between components. Billing from the same practice creates a duplicate billing error that produces automatic denial.
- Overcoding limited echo as complete: Code 93306 requires all standard cardiac views with full measurements. Consequently, if any standard view is missing, code 93308 is the only defensible code to submit.
- Failing to establish medical necessity for stress tests: Payers require a supporting ICD-10 diagnosis code that explains why the stress test was medically necessary. Submitting a stress test claim with only a screening diagnosis routinely produces a medical necessity denial.
HS MED Solutions conducts quarterly cardiology coding audits for all clients to identify these errors before they become denials or post-payment audit findings. Contact us today at info@hsmedsolutions.com or call 845-481-1953 to schedule a free cardiology billing review.
Conclusion
Cardiology CPT codes are not static reference data. They change every January, and 2026 brought more changes than any recent year. Specifically, the restructuring of PCI codes, including the deletion of six add-on codes and the introduction of 92930 and 92945, requires every cardiology billing team to update charge masters, retrain coders, and review EHR code libraries before submitting any PCI claim this year.
Furthermore, the new AI-assisted plaque analysis code 75577, the revised RPM threshold for 99454, and the new real-time monitoring code 99470 all represent genuine new revenue opportunities. However, each also carries new documentation requirements that your team must meet to support reimbursement. Therefore, correct cardiology billing codes are not only a billing task, but they are a compliance requirement and a revenue protection strategy.
Additionally, the modifier rules, bundling edits, and documentation requirements that surround cardiology CPT codes demand ongoing education, not a one-time update. As a result, practices that invest in regular coding audits, quarterly NCCI edit reviews, and a specialized cardiology billing partner consistently outperform those that do not. At HS MED Solutions, our cardiology billing team stays current with every CPT update, CMS policy change, and payer requirement throughout the year. Consequently, our clients submit cleaner claims, collect more revenue, and face fewer denials than national benchmarks. Contact us today to learn more about our cardiology billing services.
Ready to ensure your cardiology CPT codes are correct for 2026? Contact HS MED Solutions at info@hsmedsolutions.com or call 845-481-1953. We offer a free cardiology billing analysis for new clients.
Cardiology CPT Codes: Frequently Asked Questions
What is the most commonly used cardiology CPT code?
Code 93000, the complete ECG with interpretation and report, is among the most frequently billed cardiology billing codes in outpatient practice. Additionally, 93306 (complete transthoracic echocardiography) and 93015 (complete cardiovascular stress test) rank among the highest-volume cardiovascular CPT codes nationwide. However, the highest-value codes by reimbursement are typically cardiac catheterization codes (93451 to 93461), interventional codes (92920 to 92945), and electrophysiology ablation codes (93651 to 93657).
What CPT code range covers most cardiology services?
The primary cardiology CPT codes range from 92920 to 93799, covering PCI, echocardiography, stress testing, cardiac catheterization, electrophysiology, and cardiac rehabilitation. Furthermore, cardiology billing codes also appear in nuclear medicine (78451 to 78499), radiology (75571 to 75577 for cardiac CT), surgical sections for device implantation, and E&M sections for office and inpatient visits. Therefore, a cardiologist’s charge ticket may reference four separate CPT sections on the same day.
What are the biggest PCI cardiology CPT code changes for 2026?
The 2026 AMA update deleted six PCI branch vessel add-on codes, specifically 92921, 92925, 92929, 92934, 92938, and 92944, and bundled that work into revised primary PCI codes. Additionally, two new cardiology billing codes were introduced: 92930 for complex PCI involving bifurcation or multiple lesions, and 92945 for chronic total occlusion revascularization. Furthermore, new code 92930 provides approximately 20% more RVU credits than standard stent code 92928, but requires specific bifurcation documentation to support billing.
How do modifiers 26 and TC work with cardiology CPT codes?
Modifier 26 is appended to a cardiology CPT code when the cardiologist provides only the interpretation of a test performed at another facility, for example, interpreting an echocardiogram performed at a hospital outpatient department. Modifier TC is appended when a facility bills only for the equipment and technical staff without the physician’s interpretation. Importantly, modifier 26 should never be appended to code 93010, because 93010 already represents the professional-only interpretation component for ECGs. Applying modifier 26 to 93010 creates a billing error.
What is the new 2026 AI cardiology CPT code?
Code 75577 is a new Category I CPT code for 2026 that covers AI-assisted coronary plaque analysis performed alongside coronary CT angiography. Previously, this service used a Category III experimental tracking code. Upgrading to Category I status means Medicare and commercial payers must now establish formal reimbursement policies for AI-assisted plaque imaging. However, cardiology practices should verify individual payer coverage before billing 75577, as implementation timelines vary across payers.
How often should cardiology practices update their CPT code reference sets?
Cardiology practices should update their CPT code libraries every January 1 when AMA updates take effect, and additionally review ICD-10 code changes every October 1. Furthermore, NCCI edit updates occur quarterly and require ongoing monitoring throughout the year. Specifically, practices should subscribe to AMA CPT update notifications, American College of Cardiology coding corner updates, and their Medicare Administrative Contractor newsletter to stay current with every change that affects cardiology billing codes throughout the year.



One Response
This comprehensive guide to 2026 Cardiology CPT codes is an excellent resource for ensuring accurate coding and efficient billing practices. Staying current with specialty-specific CPT updates helps improve compliance and optimize reimbursements.